
A soap note is a method of documentation used by healthcare providers to record important information about a patient’s medical history and current condition. The acronym “SOAP” stands for Subjective, Objective, Assessment, and Plan.
To write a soap note, follow these steps:
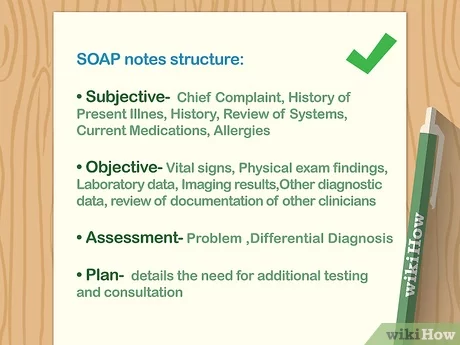
- Start with the subject line, which should include the patient’s name, the date of the visit, and the reason for the visit.
- In the subjective section, record any information provided by the patient about their symptoms, medical history, and current concerns. This should be written in the patient’s own words.
- In the objective section, record any observations made by the healthcare provider during the examination, such as vital signs, physical exam findings, and test results. This should be written in a factual and objective manner.
- In the assessment section, interpret the information gathered in the subjective and objective sections to reach a diagnosis or identify any further testing that may be needed.
- In the plan section, outline the steps that will be taken to address the patient’s concerns and manage their condition, including any medications that will be prescribed, referrals to specialists, and follow-up appointments.
It’s important to remember that soap notes should be written in a clear and concise manner, using medical terminology where appropriate. The goal is to provide a complete and accurate record of the patient’s visit that can be easily understood by other healthcare providers who may be involved in the patient’s care.
SUMMARY: How to Write SOAP notes
- Start with the patient’s identifying information, including their name, age, gender, and chief complaint.
- In the subjective section, describe the patient’s symptoms and concerns, as reported by the patient.
- In the objective section, record the results of the physical examination, including any relevant medical history and vital signs.
- In the assessment section, provide a summary of the patient’s condition and any diagnostic impressions or hypotheses.
- In the plan section, outline the recommended treatment plan, including any medications, referrals, or follow-up appointments.
- In the progress section, document any changes in the patient’s condition or response to treatment.
- Include the date and the provider’s name at the end of the note.
- Review and edit the note for clarity and accuracy.
As discussed above, a SOAP note is a common format for documenting a patient’s medical history and treatment plan. It is typically used by healthcare providers to communicate important information about a patient’s condition, treatment, and progress.
Here are some examples of SOAP notes:
Patient: Jane Doe Date: December 7, 2022
Subjective: Jane reports feeling tired and having a headache. She has been experiencing difficulty sleeping and has noticed a decrease in her energy levels over the past week. She has a history of anxiety and depression.
Objective: Jane’s vital signs are within normal limits. She appears tired and reports a mild headache. Her mood is slightly depressed and she reports feeling anxious.
Assessment: Jane is experiencing symptoms of fatigue and a mild headache, likely related to her history of anxiety and depression.
Plan:
- Prescribe medication to help with anxiety and depression
- Recommend therapy to address underlying issues contributing to symptoms
- Follow up with Jane in one week to monitor progress and adjust treatment plan as needed
Here are some examples of SOAP notes:
- Patient Name: Jane Doe Date of Visit: 2/15/2021
Chief Complaint: Patient is experiencing chest pain and shortness of breath.
Subjective: Patient reports chest pain that began suddenly while exercising. Pain is described as sharp and radiating to the left arm. Shortness of breath is also present. Patient has a history of hypertension and hyperlipidemia.
Objective:
- Blood pressure: 150/95 mmHg
- Heart rate: 104 bpm
- Respiratory rate: 24 breaths/minute
- Lungs: Clear to auscultation bilaterally
- Cardiac: Regular rate and rhythm, no murmurs or gallops
Assessment: Acute coronary syndrome.
Plan:
- Administer sublingual nitroglycerin
- Obtain ECG
- Initiate aspirin therapy
- Discuss need for hospitalization with patient
- Patient Name: John Smith Date of Visit: 1/2/2021
Chief Complaint: Patient is experiencing joint pain and swelling in the hands and wrists.
Subjective: Patient reports worsening joint pain and swelling in the hands and wrists over the past several months. Pain is described as aching and is worse with activity. Patient reports no recent injuries or trauma.
Objective:
- Joints: Swelling and tenderness in the hands and wrists
- Range of motion: Limited in the hands and wrists
- Musculoskeletal: No palpable warmth or deformities
Assessment: Rheumatoid arthritis.
Plan:
- Prescribe nonsteroidal anti-inflammatory drug (NSAID)
- Refer to rheumatologist for further evaluation and management
- Discuss use of heat and physical therapy for symptom relief.
 WRITE MY ESSAY NOW!
WRITE MY ESSAY NOW!Find online help in writing essays, research papers, term papers, reports, movie reviews, annotated bibliographies, speeches/presentations, projects, presentations, dissertation services, theses, research proposals, essay editing, proofreading, Book reviews, article reviews, formatting, personal statements, admission essays, scholarship essays, application papers, among others.